
At the beginning of this project, PET/MRI scanners that were capable of abdominal imaging were not available. For this, it was unclear if a retrospective, software based image registration between FDG-PET and MRI might be sufficient.
The following text is an excerpt of the publication
Kiefer, A., T. Kuwert, D. Hahn, J. Hornegger, M. Uder, and P. Ritt. "Anatomical accuracy of abdominal lesion localization." Nuklearmedizin 50 (2011): 147-154.
Aim:
Software-based image registration can improve the diagnostic value of imaging procedures and is an alternative to hybrid scanners. The aim of this study was to evaluate the anatomical accuracy of automatic rigid image registration of independently acquired datasets of positron emission tomography with F-18-deoxyglucose and abdominal magnetic resonance imaging.
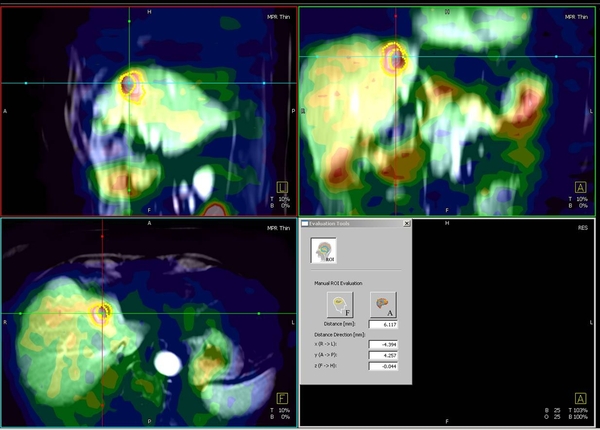
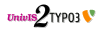
Figure 1: Example image of delineated tumour contours in PET and MRI.
Methods:
Analyses were performed on 28 abdominal lesions from 20 patients. The PET data were obtained using a stand-alone PET camera in 14 cases and a hybrid PET/CT scanner in 9 cases. The abdominal T1- and T2- weighted MRI scans were acquired on 1.5 T MRI scanners. The mean time interval between MRI and PET was 7.3 days (0-28 days). Automatic rigid registration was carried out using a self-developed registration tool integrated into commercial available software (InSpace for Siemens Syngo). Distances between the centres of gravity of 28 manually delineated neoplastic lesions represented in PET and MRI were measured in X-, Y-, and Z-direction (Example shown in Figure 1). The intra- (intraclass correlation 0.94) and inter- (intraclass correlation 0.86) observer repeatability were high.
Results:
The average distance in all MRI sequences was 5.2 ± 7.6 mm in X-direction, 4.0 ± 3.7 mm in Y-direction and 6.1 ± 5.1 mm in Z-direction. There was a significantly higher misalignment in Z-direction (p<0.05). The misalignment was not significantly different for the registration of T1- and T2- weighted sequences (p=0.7).
Conclusion:
The misalignment between FDG-PET and abdominal MRI registered using an automated rigid registration tool was comparable to data reported for software-based fusion between PET and CT. Although this imprecision may not affect diagnostic accuracy, it is not sufficient to allow for pixel-wise integration of MRI and PET information.
The comparison of our results to those published in the literature showed that the magnitude of the TRE between PET and MRI is in the range of the results reported for retrospective registration between PET and CT (2,4) but not as good as for hybrid machines (1,2) (Figure 2). Furthermore the accuracy of retrospective registration between PET and MRI in sarcoma patients was not considerably different from ours (3) (Figure 3).
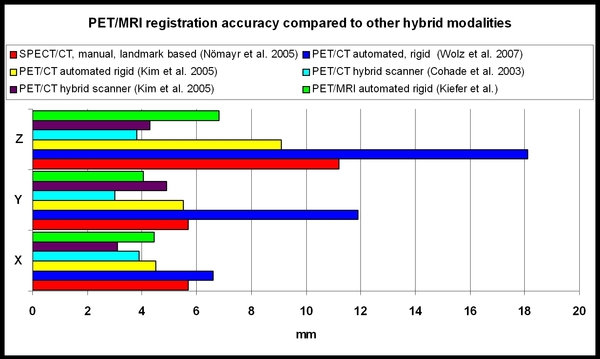
Figure 2: Comparison of misalignment for PET/MRI and other multimodal devices reported from literature.
Figure 3: Comparison of misalignment for PET/MRI reported from literature.
References:
- Cohade C, Osman M, Marshall LT, Wahl RL. PET-CT: accuracy of PET and CT spatial registration of lung lesions. European Journal of Nuclear Medicine and Molecular Imaging 2003;30:721-726
- Kim JH, Czernin J, Allen-Auerbach MS, et al. Comparison between F-18-FDG PET, in-line PET/CT, and software fusion for restaging of recurrent colorectal cancer. J Nucl Med 2005;46:587-595
- Somer EJ, Benatar NA, O'Doherty MJ, Smith MA, Marsden PK. Use of the CT component of PET-CT to improve PET-MR registration: demonstration in soft-tissue sarcoma. Phys Med Biol 2007;52:6991-7006
- Wolz G, Nömayr A, Hothorn T, et al. Anatomical accuracy of interactive and automated rigid registration between X-ray CT and FDG-PET. Nuklearmedizin-Nuclear Medicine 2007;46:43-48