
Contact



Address
Chair of Computer Science 5 (Pattern Recognition)
Martensstrasse 3
91058 Erlangen
Germany
Powered by

Dr.-Ing. Alexander Brost
Alumnus of the Pattern Recognition Lab of the Friedrich-Alexander-Universität Erlangen-Nürnberg
WARNING: All material on this website, including papers, text, figures, and graphics is covered by Copyright © unless otherwise stated. You may browse them at your convenience (in the same spirit as you may read a journal or a proceeding article in a public library). Retrieving, copying, or distributing these files, however, may violate the copyright protection law. We recommend that the user abides international law in accessing this directory.
 here
herePublications in 2012
SPIE Medical Imaging 2012: Image-Guided Procedures, Robotic Interventions, and Modeling, Vol. 8316, pp. 83162V, 2012
 |
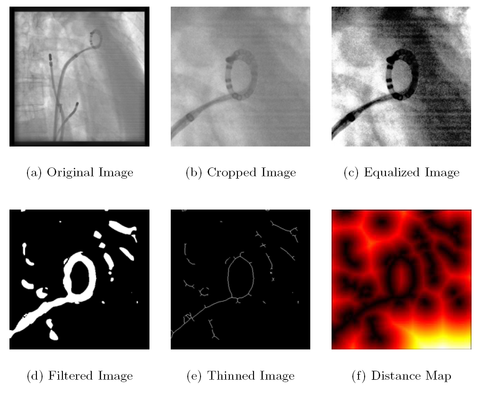
A. Brost, F. Bourier, A. Wimmer, M. Koch, A. Kiraly, R. Liao, K. Kurzidim, J. Hornegger, N. Strobel
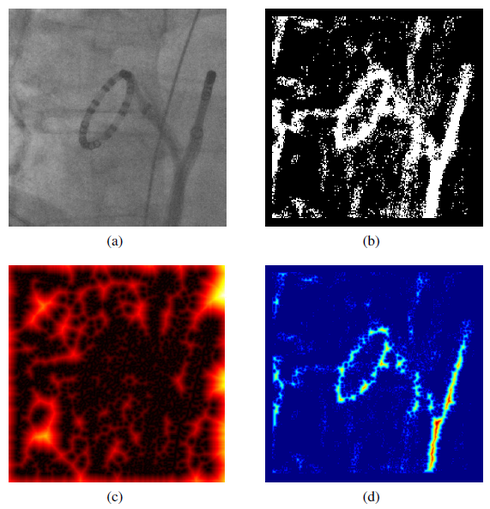
Atrial fibrillation (AFib) has been identified as a major cause of stroke. Radiofrequency catheter ablation has become an increasingly important treatment option, especially when drug therapy fails. Navigation under X-ray can be enhanced by using augmented fluoroscopy. It renders overlay images from pre-operative 3-D data sets which are then fused with X-ray images to provide more details about the underlying soft-tissue anatomy. Unfortunately, these fluoroscopic overlay images are compromised by respiratory and cardiac motion. Various methods to deal with motion have been proposed. To meet clinical demands, they have to be fast. Methods providing a processing frame rate of 3 frames-per-second (fps) are considered suitable for interventional electrophysiology catheter procedures if an acquisition frame rate of 2 fps is used. Unfortunately, when working at a processing rate of 3 fps, the delay until the actual motion compensated image can be displayed is about 300 ms. By using a novel approach involving a 3-D catheter model, catheter segmentation and a distance transform, we can speed up motion compensation to 20 fps which results in a display delay of only 50 ms on a standard workstation for medical applications. Our method uses a constrained 2-D/3-D registration to perform catheter tracking, and it obtained a 2-D tracking error of 0.61 mm.
Full paper available  here.
here.
Publications in 2011
MICCAI 2011, LNCS, Vol. 6891, pp. 540–547
 |
A. Brost, W. Wu, M. Koch, A. Wimmer, T. Chen, R. Liao, J. Hornegger, N. Strobel
Catheter ablation of atrial fibrillation has become an accepted treatment option if a patient no longer responds to or tolerates drug therapy. A main goal is the electrical isolation of the pulmonary veins attached to the left atrium. Catheter ablation may be performed under fluoroscopic image guidance. Due to the rather low soft-tissue contrast of X-ray imaging, the heart is not visible in these images. To overcome this problem, overlay images from pre-operative 3-D volumetric data can be used to add anatomical detail. Unfortunately, this overlay is compromised by respiratory and cardiac motion. In the past, two methods have been proposed to perform motion compensation. The first approach involves tracking of a circumferential mapping catheter placed at an ostium of a pulmonary vein. The second method relies on a motion estimate obtained by localizing an electrode of the coronary sinus (CS) catheter. We propose a new motion compensation scheme which combines these two methods. The effectiveness of the proposed method is verified using 19 real clinical data sets. The motion in the fluoroscopic images was estimated with an overall average error of 0.55 mm by tracking the circumferential mapping catheter. By applying an algorithm involving both the CS catheter and the circumferential mapping catheter, we were able to detect motion of the mapping catheter from one pulmonary vein to another with a false positive rate of 5.8 %.
Full paper available here.
IPCAI 2011, LNCS, Vol. 6689, 2011, pp. 133-144
 |
A. Brost, A. Wimmer, R. Liao, J. Hornegger, N. Strobel
Fluoroscopic overlay images rendered from pre-operative volumetric data can provide additional guidance for physicians during catheter ablation procedures for treatment of atrial fibrillation (AFib). As these overlay images are compromised by cardiac and respiratory motion, motion compensation methods have been proposed. The approaches so far either require simultaneous biplane imaging for 3-D motion compensation or, in case of mono-plane X-ray imaging, provide only a limited 2-D functionality. To overcome the downsides of the previously suggested methods, we propose a new approach that facilitates full 3-D motion compensation even if only mono-plane X-ray views are available. To this end, we use constrained model-based 2-D/3-D registration to track a
circumferential mapping catheter which is commonly used during AFib catheter ablation procedures. Our approach yields an average 2-D tracking error of 0.6 mm and an average 3-D tracking error of 2.1 mm.
Full paper available here.
18th IEEE International Conference on Image Processing, Brussels, Belgium, 11.09. - 14.09.2011, pp. 989-992, 2011
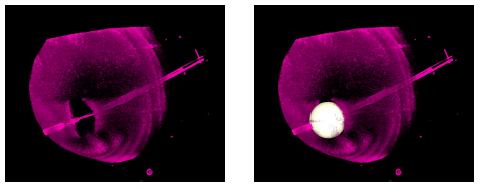 |
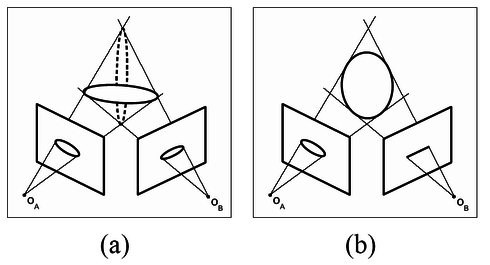
A. Kleinoeder, A. Brost, F. Bourier, M. Koch, K. Kurzidim, J. Hornegger, N. Strobel
Atrial fibrillation is a major cause of stroke. Its treatment is performed under fluoroscopic image guidance. Augmented fluoroscopy has become a useful tool during the ablation procedure for navigation under X-ray. Unfortunately, current navigation systems do not provide tools to localize and visualize a cryo-balloon catheters in 3-D. This is why we present a new approach to reconstruct the cryo-ballon catheter, modeled as a sphere, from two views. The reconstruction result can then be overlayed onto live fluoroscopic images during the procedure. In simulation studies, we compared our technique to a reference method. While both methods worked equally well on noise-free data, we found our method more reliable if the input data was affected by noise. For example, in the presence of noise with a standard deviation of 4 mm, our maximum 3-D reconstruction error was less than 1 mm.
Full paper available here.
SPIE Medical Imaging 2011: Visualization, Image-Guided Procedures, and Modeling, Vol. 7964 2011, pp. 79641O
 |
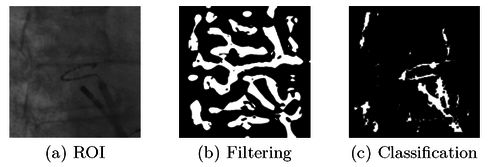
A. Brost, A. Wimmer, R. Liao, J. Hornegger, N. Strobel
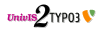
The treatment of atrial fibrillation has gained increasing importance in the field of computer-aided interventions. State-of-the-art treatment involves the electrical isolation of the pulmonary veins attached to the left atrium under fluoroscopic X-ray image guidance. Due to the rather low soft-tissue contrast of X-ray fluoroscopy, the heart is difficult to see. To overcome this problem, overlay images from pre-operative 3-D volumetric data can be used to add anatomical detail. Unfortunately, these overlay images are static at the moment, i.e., they do not move with respiratory and cardiac motion. The lack of motion compensation may impair X-ray based catheter navigation, because the physician could potentially position catheters incorrectly. To improve overlay-based catheter navigation, we present a novel two stage approach for respiratory and cardiac motion compensation. First, a cascade of boosted classifiers is employed to segment a commonly used circumferential mapping catheter which is firmly fixed at the ostium of the pulmonary vein during ablation. Then, a 2-D/2-D model-based registration is applied to track the segmented mapping catheter. Our novel hybrid approach was evaluated on 10 clinical data sets consisting of 498 fluoroscopic monoplane frames. We obtained an average 2-D tracking error of 0.61 mm, with a minimum error of 0.26 mm and a maximum error of 1.62 mm. These results demonstrate that motion compensation using registration-based catheter tracking is both feasible and accurate. Using this approach, we can only estimate in-plane motion. Fortunately, compensating for this is often sufficient for EP procedures where the motion is governed by breathing.
Full paper available here.
SPIE Medical Imaging 2011: Visualization, Image-Guided Procedures, and Modeling, Vol. 7964 2011, pp. 79641P
 |
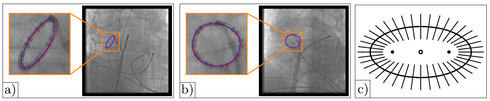
A. Brost, F. Bourier, L. Yatziv, M. Koch, J. Hornegger, N. Strobel, K. Kurzidim
Atrial fibrillation is the most common heart arrhythmia and a leading cause of stroke. The treatment option of choice is radio-frequency catheter ablation, which is performed in electrophysiology labs using C-Arm X-ray systems for navigation and guidance. The goal is to electrically isolate the pulmonary vein-left atrial junction thereby rendering myocardial fibers responsible for induction and maintenance of AF inactive. The use of overlay images for fluoroscopic guidance may improve the quality of the ablation procedure, and can reduce procedure time. Overlay images, acquired using CT, MRI, or C-arm CT, can add soft-tissue information, otherwise not visible under X-ray. MRI can be used to image a wide variety of anatomical details without ionizing radiation. In this paper, we present a method to register a 3-D MRI volume to 2-D biplane X-ray images using the coronary sinus. Current approaches require registration of the overlay images to the fluoroscopic images to be performed after the trans-septal puncture, when contast agent can be administered. We present a new approach for registration to align overlay images before the trans-septal puncture. To this end, we manually extract the coronary sinus from pre-operative MRI and register it to a multi-electorde catheter placed in the coronary sinus.
Publications in 2010
Medical Image Analysis 14 (5) pp. 695-706, 2010
 |
A. Brost, R. Liao, N. Strobel, and J. Hornegger
In many cases, radio-frequency catheter ablation of the pulmonary veins attached to the left atrium still involves fluoroscopic image guidance. Twodimensional X-ray navigation may also take advantage of overlay images derived from static pre-operative 3-D volumetric data to add anatomical details otherwise not visible under X-ray. Unfortunately, respiratory motion may impair the utility of static overlay images for catheter navigation. We developed a novel approach for image-based 3-D motion estimation and compensation as a solution to this problem. It is based on 3-D catheter tracking which, in turn, relies on 2-D/3-D registration. To this end, a bi-plane C-arm system is used to take X-ray images of a special circumferential mapping catheter from two directions. In the first step of the method, a 3-D model of the device is reconstructed. Three-dimensional respiratory motion at the site of ablation is then estimated by tracking the reconstructed catheter model in 3-D based on bi-plane fluoroscopy. Phantom data and clinical data were used to assess model-based catheter tracking. Our phantom experiments yielded an average 2-D tracking error of 1.4 mm and an average 3-D tracking error of 1.1 mm. Our evaluation of clinical data sets comprised 469 bi-plane fluoroscopy frames (938 monoplane fluoroscopy frames). We observed an average 2-D tracking error of 1.0 mm ± 0.4 mm and an average 3-D tracking error of 0.8 mm ± 0.5 mm. These results demonstrate that model-based motion-compensation based on 2-D/3-D registration is both feasible and accurate.
Full paper available here.
SPIE Medical Imaging 2010, 2010, pp. 762507
 |
A. Brost, R. Liao, J. Hornegger, and N. Strobel
Atrial fibrillation is the most common sustained heart arrhythmia and a leading cause of stroke. Its treatment by radio-frequency catheter ablation, performed using fluoroscopic image guidance, is gaining increasingly more importance. Two-dimensional fluoroscopic navigation can take advantage of overlay images derived from pre-operative 3-D data to add anatomical details otherwise not visible under X-ray. Unfortunately, respiratory motion may impair the utility of these static overlay images for catheter navigation. We developed an approach for image-based 3-D motion compensation as a solution to this problem. A bi-plane C-arm system is used to take X-ray images of a special circumferential mapping catheter from two directions. In the first step of the method, a 3-D model of the device is reconstructed. Three-dimensional respiratory motion at the site of ablation is then estimated by tracking the reconstructed catheter model in 3-D. This step involves bi-plane fluoroscopy and 2-D/3-D registration. Phantom data and clinical data were used to assess our model-based catheter tracking method. Experiments involving a moving heart phantom yielded an average 2-D tracking error of 1.4 mm and an average 3-D tracking error of 1.1 mm. Our evaluation of clinical data sets comprised 469 bi-plane fluoroscopy frames (938 monoplane fluoroscopy frames). We observed an average 2-D tracking error of 1.0 mm ± 0.4 mm and an average 3-D tracking error of 0.8 mm ± 0.5 mm. These results demonstrate that model-based motion-compensation based on 2-D/3-D registration is both feasible and accurate.
Full paper available here.
Lecture Notes in Computer Science, Vol. 6376, 2010, pp. 293-302
 |
A. Brost, A. Wimmer, R. Liao, J. Hornegger, and N. Strobel
Atrial fibrillation is the most common sustained arrhythmia. One important treatment option is radio-frequency catheter ablation (RFCA) of the pulmonary veins attached to the left atrium. RFCA is usually performed under fluoroscopic (X-ray) image guidance. Overlay images computed from pre-operative 3-D volumetric data can be used to add anatomical detail otherwise not visible under X-ray. Unfortunately, current fluoro overlay images are static, i.e., they do not move synchronously with respiratory and cardiac motion. A filter-based catheter tracking approach using simultaneous biplane fluoroscopy was previously presented. It requires localization of a circumferential tracking catheter, though. Unfortunately, the initially proposed method may fail to accommodate catheters of different size. It may also detect wrong structures in the presence of high background clutter. We developed a new learning-based approach to overcome both problems. First, a 3-D model of the catheter is reconstructed. A cascade of boosted classifiers is then used to segment the circumferential mapping catheter. Finally, the 3-D motion at the site of ablation is estimated by tracking the reconstructed model in 3-D from biplane fluoroscopy. We compared our method to the previous approach using 13 clinical data sets and found that the 2-D tracking error improved from 1.0 mm to 0.8 mm. The 3-D tracking error was reduced from 0.8 mm to 0.7 mm.
Full paper available here.
8th Interventional MRI Symposium, 2010, pp. 311-313
 |
F. Bourier, A. Brost, L. Yatziv, J. Hornegger, N. Strobel, and K. Kurzidim
Atrial fibrillation (Afib) is the most common heart arrhythmia and a leading cause of stroke. The treatment option is radio-frequency catheter ablation (RFCA). RFCA is performed in electrophysiology (EP) labs using C-Arm X-ray systems for navigation and guidance. The goal is to electrically isolate the pulmonary vein-left atrial junction thereby rendering myocardial fibers responsible for induction and maintenance of AF inactive. The use of overlay images for fluoroscopic guidance may improve the quality of the ablation, and it can reduce procedure time. Overlay images, acquired using CT, MRI, or C-arm CT, can add soft-tissue information otherwise not visible under X-ray. MRI can be used to image a wide variety of anatomical details without ionizing radiation. In this paper, we show how to register 3-D MRI volumes to 2-D X-ray images based on the coronary sinus.
Full paper available here.
WBIR 2010, LNCS, Vol. 6204, 2010, pp. 234-245
 |
A. Brost, R. Liao, J. Hornegger, and N. Strobel
Radio-frequency catheter ablation (RFCA) has become an accepted treatment option for atrial fibrillation (Afib). RFCA of Afib involves isolation of the pulmonary veins under X-ray guidance. For easier navigation, two-dimensional X-ray imaging may take advantage of overlay images derived from static pre-operative 3-D data set to add anatomical details which, otherwise, would not be visible under X-ray. Unfortunately, respiratory and cardiac motion may impair the utility of static overlay images for catheter navigation. We developed a system for image-based 2-D motion estimation and compensation as a solution to this problem. It is based on 2-D catheter tracking facilitated by modelbased registration of an ellipse-shaped model to fluorosocpic images. A mono-plane or a bi-plane X-ray C-arm system can be used. In the first step of the method, a 2-D model of the catheter device is computed. Respiratory and cardiac motion at the site of ablation is then estimated by tracking the catheter device in fluoroscopic images. The cost function of the registration step is based on the average distance of the model to the segmented circumferential mapping catheter using a distance map. In our experiments, the circumferential catheter was successfully tracked in 688 fluoroscopic images with an average 2-D tracking error of 0.59 mm ± 0.25 mm. Our presented method achieves a tracking rate of 10 frames-per-second.
Full paper available here.
Publications in 2009
Lecture Notes in Computer Science, Vol. 5761, 2009, pp. 394-401
 |
A. Brost, R. Liao, J. Hornegger, and N. Strobel
Radio-frequency catheter ablation of the pulmonary veins attached to the left atrium is usually carried out under fluoroscopy guidance. Two-dimensional X-ray navigation may involve overlay images derived from a static pre-operative 3-D volumetric data set to add anatomical details. However, respiratory motion may impair the utility of static overlay images for catheter navigation. We developed a system for image-based 3-D motion estimation and compensation as a solution to this problem for which no previous solution is yet known. It is based on 3-D catheter tracking involving 2-D/3-D registration. A biplane X-ray C-arm system is used to image a special circumferential (lasso) catheter from two directions. In the first step of the method, a 3-D model of the device is reconstructed. 3-D respiratory motion at the site of ablation is then estimated by tracking the reconstructed model in 3-D from biplane fluoroscopy. In our experiments, the circumferential catheter was tracked in 231 biplane fluoro frames (462 monoplane fluoro frames) with an average 2-D tracking error of 1.0 mm ± 0.5 mm.
Full paper available here.
MICCAI 2009 Workshop on Geometric Accuracy in Image Guided Interventions, Accuracy 2009, September 20, 2009, London, UK
 |
A. Brost, N. Strobel, L. Yatziv, W. Gilson, B. Meyer, J, Hornegger, J. Lewin, and F. Wacker
Image guided interventions often involve C-arm X-ray imaging systems. State-of-the art fluoroscopy systems not only offer 2-D Xray imaging, but they can also be used to obtain 3-D cone-beam tomographic data sets. These 3-D volumetric images can be used for image guidance and device navigation. To navigate a device with confidence, it is, however, important to know where it is with respect to the volume. We addressed this question by evaluating the geometric accuracy of 3-D X-ray image-based localization from two C-arm views. To this end a simulation study was performed first. The results of this study are compared with a phantom experiment involving a real C-arm system. The phantom design comprised five point-like objects arranged in such a way that they could be distinguished in all possible viewing directions. The same point configuration was used for simulation study and experiment. For the simulation study, these five 3-D points were forward projected assuming an ideal C-arm imaging geometry. The resulting point coordinates at the detector were then disturbed by Gaussian noise (standard deviation: 1.232 mm). Finally, 3D point localization was performed by triangulation from two views again assuming an ideal C-arm system geometry. The error for two imaging views was calculated as the Euclidean distance between the localized and the original 3-D points and averaged over the five objects. For the (real) experiment, the idealized projection matrices were replaced by actual projection matrices returned by the system. The simulation results yielded a minimal localization error of 0.81 mm. In the experiment, a minimal error of 0.99 mm was achieved.
Full paper available here.
Medical Imaging 2009, Visualization, Image-Guided Procedures, and Modeling
 |
A. Brost, N. Strobel, L. Yatziv, W. Gilson, B. Meyer, J. Hornegger, J. Lewin, and F. Wacker
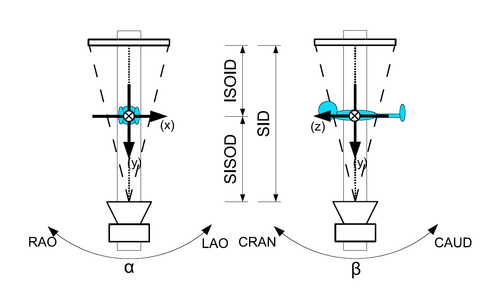
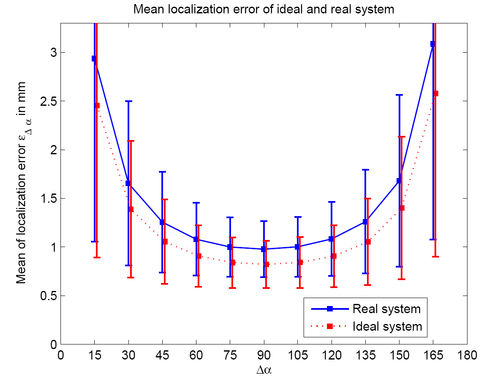
C-arm X-ray imaging devices are commonly used for minimally invasive cardiovascular or other interventional procedures. Calibrated state-of-the-art systems can, however, not only be used for 2D imaging but also for three-dimensional reconstruction either using tomographic techniques or even stereotactic approaches. To evaluate the accuracy of X-ray object localization from two views, a simulation study assuming an ideal imaging geometry was carried out first. This was backed up with a phantom experiment involving a real C-arm angiography system. Both studies were based on a phantom comprising five point objects. These point objects were projected onto a flat-panel detector under different C-arm view positions. The resulting 2D positions were perturbed by adding Gaussian noise to simulate 2D point localization errors. In the next step, 3D point positions were triangulated from two views. A 3D error was computed by taking differences between the reconstructed 3D positions using the perturbed 2D positions and the initial 3D positions of the five points. This experiment was repeated for various C-arm angulations involving angular differences ranging from 15o to 165o. The smallest 3D reconstruction error was achieved, as expected, by views that were 90o degrees apart. In this case, the simulation study yielded a 3D error of 0.82 mm ± 0.24 mm (mean ± standard deviation) for 2D noise with a standard deviation of 1.232 mm (4 detector pixels). The experimental result for this view configuration obtained on an AXIOM Artis C-arm (Siemens AG, Healthcare Sector, Forchheim, Germany) system was 0.98 mm ± 0.29 mm, respectively.
These results show that state-of-the-art C-arm systems can localize instruments with millimeter accuracy, and that they can accomplish this almost as well as an idealized theoretical counterpart. High stereotactic localization accuracy, good patient access, and CT-like 3D imaging capabilities render state-of-the-art C-arm systems ideal devices for X-ray based minimally invasive procedures.
Full paper available here.