
Contact



Address
Chair of Computer Science 5 (Pattern Recognition)
Martensstrasse 3
91058 Erlangen
Germany
Powered by

Dr.-Ing. Alexander Brost
Alumnus of the Pattern Recognition Lab of the Friedrich-Alexander-Universität Erlangen-Nürnberg
Real-Time Circumferential Mapping Catheter Tracking for Motion Compensation in Atrial Fibrillation Ablation Procedures
 Alexander Brost, Felix Bourier,
Alexander Brost, Felix Bourier,  Andreas Wimmer, Martin Koch, Atilla Kiraly, Rui Liao, Klaus Kurzidim, Joachim Hornegger, and Norbert Strobel
Andreas Wimmer, Martin Koch, Atilla Kiraly, Rui Liao, Klaus Kurzidim, Joachim Hornegger, and Norbert Strobel
Atrial fibrillation (AFib) is the most common heart arrhythmia, and leads to an increased risk of stroke for the patients. Since the first treatment approaches using radio-frequency ablation, this method has now become an accepted treatment option, in particular when drug therapy fails. Catheter ablation procedures are performed in electrophysiology (EP) labs usually equipped with modern C-arm X-ray systems. Augmented fluoroscopy, overlaying 2-D renderings obtained from either CT, MR, or C-arm CT 3-D data sets onto live fluoroscopic images, can facilitate more precise real-time catheter navigation and also reduce radiation. Unfortunately, catheter navigation under augmented fluoroscopy is compromised by cardiac and respiratory motion. A first approach to tackle this problem by providing a motion compensated overlay was proposed here. It involved tracking of commonly used circumferential mapping catheters. As AFib therapy takes place in the vicinity of the circumferential mapping catheter, tracking the catheter can be assumed to capture the motion of the relevant treatment region correctly if the device has been firmly positioned. Fortunately, we can count on the physicians to provide a stable wall contact, as it is in their best interest. Otherwise complete isolation of the pulmonary veins (PVs) may fail due to undetected residual PV-atrial electrical connections. The initially proposed method generated a 3-D model of the catheter and applied an unconstrained 2-D/3-D registration to register the catheter model to biplane fluoroscopy images. This work was extended regarding robustness using a learning-based catheter segmentation. The approach was also modified to work on monoplane systems as well, see here. This approach does not require simultaneously biplane fluoroscopy but instead uses a constrained 2-D/3-D registration to achieve motion compensation if only monoplane acquisitions are used at a biplane system. We extended this method to achieve real-time capability, even outperforming other motion compensation approaches.
The proposed method comprises three main steps. First, a 3-D model of the mapping catheter is generated. Second, the catheter is segmented in 2-D X-ray images using a classifier. The segmentation result is refined next. The main difference to previous approaches is that our method does not use the a thinning algorithm. Finally, the catheter is tracked relying on 2-D/3-D registration of the 3-D catheter model to the 2-D X-ray images. The resulting motion information can be used to adjust the fluoroscopic overlay accordingly. Below, these steps are explained in more detail here.
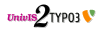
For the evaluation of the proposed method, 13 clinical biplane sequences were available. Biplane sequences were required to calculate an estimate for the 3-D error of our motion compensation approach. The 2-D tracking error was calculated as the average distance between the motion-compensated catheter model and the manually segmented mapping catheter. Manual segmentation was supervised by a cardiologist. This distance was averaged over all frames of a particular sequence to arrive at an overall tracking error for each sequence. Our proposed method achieved a 2-D tracking error of 0.61 mm +/- 0.45 mm. The 3-D tracking error was evaluated by comparing the 3-D motion vector obtained from our constrained motion compensation approach to a 3-D motion vector obtained from the biplane sequences. The 3-D error turned out to be 2.10 mm +/- 1.26 mm. The results are given below.
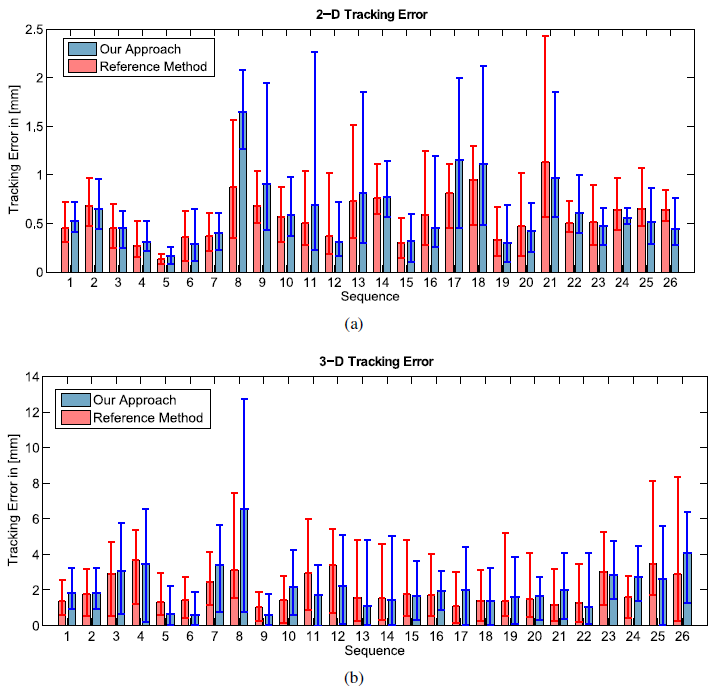 |
We developed a method for respiratory and cardiac motion compensation for use in radiofrequency catheter ablation of atrial fibrillation that is capable of real-time processing. It outperforms a different approach for motion compensation and its accuracy. Although the accuracy is slightly lower than other methods, see here, the speed-up might be the key for its application as this method does not put any restrictions on the procedure regarding the acquisition frame rate. Excluding the skeletonization from the image processing pipeline has two effects. First, the processing speed increases, but at the same time, the method becomes less accurate. The difference between our method and the reference method is at most 0.74 mm or ∼ 4 pixels in the fluoroscopic image. The presented method appears to have a rather high 3-D error, however this is because we try to estimate 3-D motion from a single X-ray view. It is possible to reduce the 3-D error by resorting to simultaneous biplane X-ray imaging, see here, but this increases the X-ray dose for patient and physician. We consider our method as another step towards a fully integrated software guidance application for electrophysiology procedures, especially atrial fibrillation ablation procedures, that accommodates physicians' needs as much as possible. Our implementation of the reference method, see here, was found to be able to process at least 10 frames-per-second (fps). Our new approach achieved a minimum frame rate of 20 fps.
Full paper available here.
